
By Fernando Vidal
 |
| Image courtesy of Wikimedia Commons. |
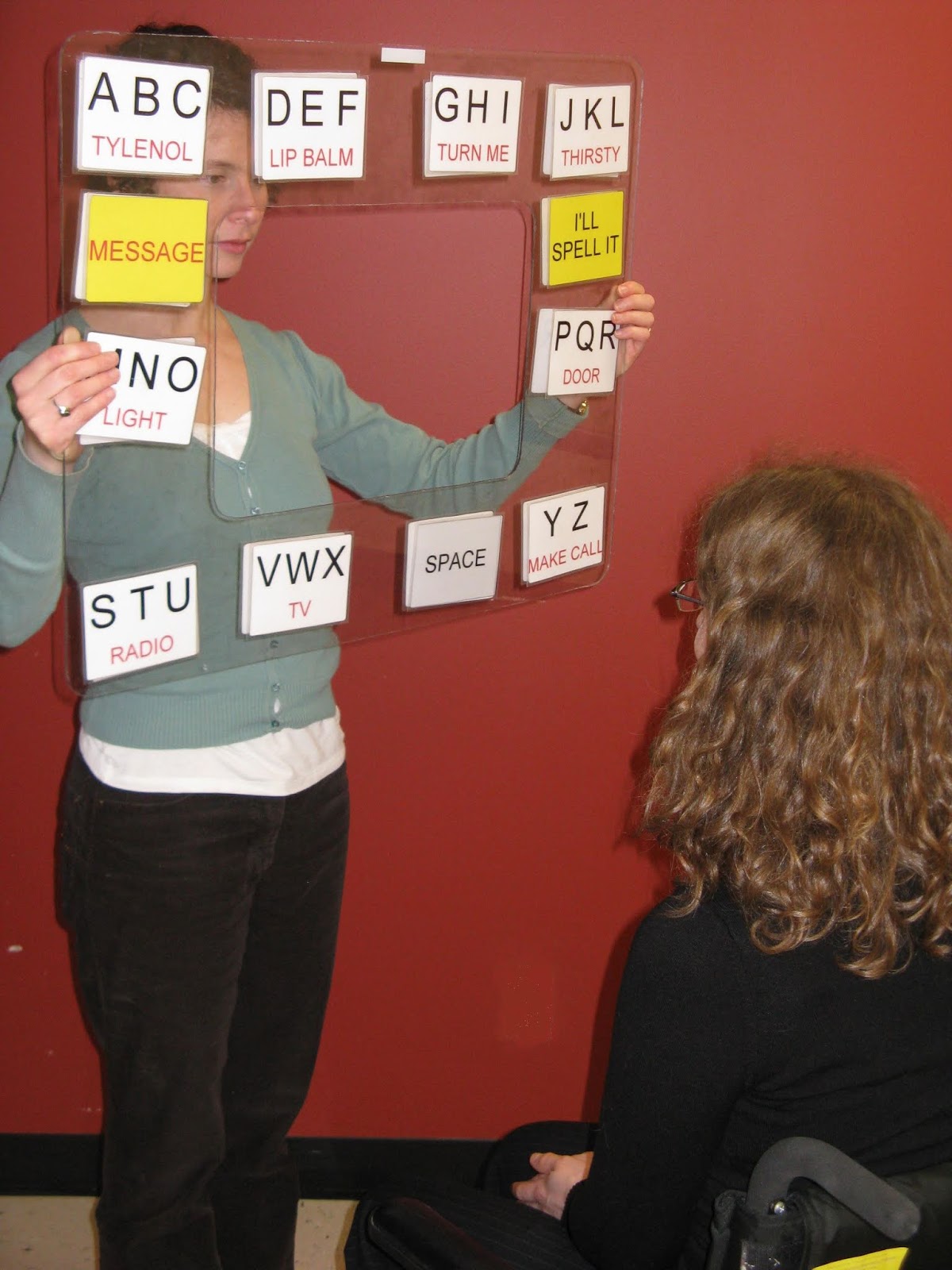
The main features of the locked-in syndrome (LIS) explain its name: persons in LIS are tetraplegic and cannot speak, but have normal visual perception, consciousness, cognitive functions and bodily sensations. They are “locked in” an almost entirely motionless body. A condition of extremely low prevalence identified and named in 1966, LIS most frequently results from a brainstem stroke or develops in the advanced stage of a neurodegenerative disease such as amyotrophic lateral sclerosis (ALS), which affects the motor neuron system and leads to paralysis. LIS presents three forms. In total or complete LIS (CLIS), patients lack all mobility; in classic LIS, blinking or vertical eye movements are preserved; in incomplete LIS, other voluntary motion is possible. Mortality is high in the early phase of LIS of vascular origin, but around 80% of patients who become stable live ten years and 40% live twenty years after entering the locked-in state. Persons who are locked-in as consequence of stroke or traumatic injury sometimes evolve from classic to incomplete LIS. They can usually communicate via blinking or vertical eye movement, by choosing letters from an alphabet spell board. When additional movements are regained, they facilitate the use of a computer. It is hoped that brain-computer interfaces (BCI) will enable CLIS patients to communicate too.
In January 2017, under the title “Groundbreaking system allows locked-in syndrome patients to communicate,” The Guardian reported on a study demonstrating that four ALS patients, two in complete LIS and two entering the condition, learned to respond to questions in a way that could be decoded by measuring frontocentral oxygenation changes detected with functional near infrared spectroscopy. Niels Birbaumer, well-known for his pioneering work on BCIs, told the journal that such a result (which has since been questioned) was “the first sign that completely locked-in syndrome may be abolished forever, because with all of these patients we can now ask them the most critical questions in life.”
Yet what do we know about how locked-in persons envisage such critical questions and relate them to the extreme existential situation in which they find themselves? Rather little. A systematic phenomenology, in the sense of a description and analysis of experience as lived by locked-in persons themselves, has not yet been undertaken. It deserves to exist along mainstream, more clinical and quantitative approaches to the question, “What is it like to be conscious but paralyzed and voiceless?”
Speaking of a “happy majority” of locked-in persons may be exaggerated given the response rates to quality of life (QOL) surveys. At the same time, the existing research shows that many locked-in persons report subjective wellbeing and a relatively satisfactory QOL level that stays stable over time. As a population they display low rates of depression, suicidal thoughts, euthanasia requests, and do-not-resuscitate orders. Most respondents to a ground-breaking closed-ended questionnaire about body and personal identity in LIS said they felt they were essentially the same as before entering the locked-in state, reporting a continuous experienced identity when they accepted their bodily changes, and a discontinuous one when they did not. The body, though paralyzed, remains a strong component of identity. The phenomenological dynamics of such relationship to the body has been explored in cases of profound paralysis due to ALS or multiple sclerosis, but not yet for LIS.
 |
| Image courtesy of pxhere. |
Illness, notes philosopher Havi Carel, is a “limit case of embodied experience.” As an extreme instance of that limit, LIS offers a unique opportunity to investigate on a real-life basis central questions related to notions and practices of personhood and embodiment in the realm of values, beliefs and experiences. These questions, concerning for example the relationships between mind and body, self and other, autonomy and dependency, life in health and illness, or the criteria for ascertaining rights and obligations, are at the heart of significant contemporary debates in philosophy, ethics, and the practice of medicine.
In the perspective of “enactivism,” which sees the mind as embodied, embedded, extended and enacted, LIS appears as a social injury that affects the self through its impact on the individual’s capacity to engage with the social environment. Though operating in a frame that places more emphasis on first-person experience, individual self-awareness and self-narrative, a phenomenologist such as Richard Zaner also attributes a central role to the interactive, relational and communicative processes involved in locked-in individuals’ experience. Beyond their obvious practical import, communication and intersubjectivity emerge as possessing fundamental ontological significance. By describing in detail the processes they involve, phenomenology throws light on philosophical and anthropological issues. But it should also contribute to caring for persons whose lives, contrary to what healthy people and even professionals believe, are worth living – yet whose predicament and capacities have been understood in ways that may strip them of their civil and political rights. Other hitherto ignored dimensions, like gender or emotions, will have to be taken into account. The same applies to such material realities as the level of financial support from the state. These realities help explain why, for example, the use and acceptance of tracheostomy ventilation – a procedure in which a tube is inserted into a person’s windpipe through a cut in the neck to allow breathing – is more frequent in Japan than in Western countries.
A consolidating network of scholars from various disciplines in Europe, North America and Japan aims at working toward a phenomenology of LIS mainly by way of two complementary qualitative methodologies. On the one hand, the project Phenomenology of the Locked-in Syndrome analyzes locked-in persons’ autobiographical narratives. There are about thirty such narratives in Western European languages and at least as many in Japanese. A few articles discuss from a literary or phenomenological standpoint Jean-Dominique Bauby’s The Diving Bell and the Butterfly (1997), the widely translated bestseller Julian Schnabel made into a prize-winning film. But the rest of the memoirs, and the corpus as a whole, remain to be scrutinized. On the other hand, the project studies the experience of LIS by way of open-ended questionnaires and interviews with patients, caregivers and family members. Instances of this approach, also a novelty with regard to LIS, are included in a forthcoming special issue of Neuroethics entitled “The Locked-in Syndrome: Perspectives from Ethics, History and Phenomenology.” [1]
 |
| Image courtesy of Wikimedia Commons. |
The place of LIS within bioethics and neuroethics looks paradoxical. Because consciousness is preserved in LIS, and because this function is considered as the most critical standard for human personhood, there is never any doubt that locked-in individuals are fully persons. Even when they are subjected to some form of tutelage, their circumstances do not give rise to the ethical and procedural issues that are customary in connection with the disorders of consciousness (DOC). Misdiagnosis (as “vegetative”) and its dramatic consequences (the patient is no longer considered a person) have been often documented, but that does not alter the ontological status of the affected individuals. This situation explains the marginal place of LIS in bioethics and neuroethics. The challenges LIS raises – about enabling communication, the exercise of autonomy, the status of advanced directives, the validity of informed consent, or decision-making about treatment and end-of-life – are not really specific to the condition, and are ethically less knotty than in the case of DOC. Knowledge about LIS patients’ self-assessed QOL and the fact that communicative difficulties are the chief source of their suffering gives rise to a twofold moral imperative: the above-mentioned healthy people’s negative biases toward life in the locked-in state should be avoided, and everything possible has to be done to facilitate communication.
It should be possible to go beyond such considerations. The limited attention devoted to LIS in neuroethics and biomedical ethics may mirror the rarity of the syndrome, but it also reflects the modern Western primacy of (self)consciousness and autonomy as normative criteria for personhood and for defining obligations toward patients. LIS, however, highlights the extent to which communication and relationality are integral to their empirical realization. The philosophy of personhood has emphasized physical and psychological criteria to varying degrees, and the human sciences have argued for a more constitutive role for intersubjectivity and technological systems. In such a context, LIS has to be examined together with conditions, such as DOC and dementias, which more directly problematize personhood at the conceptual and practical levels. Locked-in persons’ experience invites us to explore these issues by turning the usual vantage point around – asking what LIS can do for theories, rather than what theories can do for LIS [2].
_________________

Fernando Vidal is Research Professor of ICREA (Catalan Institution for Research and Advanced Studies) and Professor at the Medical Anthropology Research Center, Rovira i Virgili University (Tarragona, Spain). A former Guggenheim Fellow, he was in 2017 elected to the Academia Europaea, and was Fellow at the Brocher Foundation (Geneva) and Visiting Professor at Ritsumeikan University (Kyoto). His most recent book, Being Brains: Making the Cerebral Subject (with F. Ortega) received the 2018 Outstanding Book Award of the International Society for the History of the Neurosciences.
Author's Notes
[1] Edited by F. Vidal, it brings together participants of the workshop Personhood and the Locked-in Syndrome (Barcelona, 2016), funded by the Catalan Institution for Research and Advanced Studies with additional support from the Víctor Grifols i Lucas Foundation. The project Phenomenology of the Locked-in Syndrome is attached to the Medical Anthropology Research Center, Rovira i Virgili University, Tarragona.
[2] This post sketches some of the issues extensively discussed in F. Vidal, “Phenomenology of the Locked-in Syndrome: An Overview and Some Suggestions” (Neuroethics, in press). https://doi.org/10.1007/s12152-018-9388-1.
Locked-in persons are scattered, and not easy to find and contact. Individuals in any country interested in collaborating with the project sketched here can write to F. Vidal, fernando.vidal@icrea.cat.
Want to cite this post?
Vidal, F. (2018). Phenomenology of the Locked-in Syndrome: Time to Move Forward. The Neuroethics Blog. Retrieved on
, from http://www.theneuroethicsblog.com/2018/10/phenomenology-of-locked-in-syndrome.html






 shown holding the tamping iron which injured him")















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}