
By Sunidhi Ramesh
 |
| A side-by-side comparison of a sea horse and the human hippocampus (Greek for sea monster). (Image courtesy of Wikimedia Commons.) |
In 1587, Venetian anatomist Julius Aranzi gave a name to the intricate, hallmark structure located in the medial temporal lobe of the human brain—the hippocampus, Greek for sea monster.
The hippocampus, often said to resemble a sea horse, has since been identified as a key player in the consolidation of information (from short-term memory to long-term memory) and in the spatial memory that allows for our day-to-day navigation. Because of its importance in learning and memory, hippocampal damage is often a culprit in varying forms of dementia, Alzheimer’s disease, short-term memory loss, and amnesia.
Since its discovery, the hippocampus has been the subject of extensive research ranging from understanding diet and exercise as cognitive modulators to demonstrating the three-step encoding, storage, and retrieval process that the structure so consistently performs. In this time, it has become apparent that the hippocampus is not only a vital structure for normal human functioning, but it is also necessary to what makes us uniquely human.
In the center of this hippocampal research are place cells, individual neurons in the hippocampus that become active when an animal “enters a particular cell-specific place in its environment.” These cells are able to collect distinctive components of an organism’s surroundings and then organize their outputs in a way that is useful for the brain to understand its own location in space.
The hippocampus, then, is a model system for neural information coordination. It uses consistently reliable coding to function like a GPS, signaling the animal’s location through a pattern of activity across a population of place cells; different cells that are active and silent at each location of an environment behave like a jumbotron, allowing the cells together to code for the animal’s current location. This ensures that whenever a cell discharges, there is (more or less) a simple and single interpretation for the animal’s position.
 |
| The human hippocampus (indicated here in red) is a bilateral structure located under the cerebral cortex in the medial temporal lobe. (Image courtesy of Wikimedia Commons.) |
A different pattern of active and silent cells signals a different location, which, ultimately, continues to chart the space the animal is in. Together, place cells act to work as the brain’s cognitive map, a mental representation of places the animal knows and is familiar with.
In order to better understand place cells, Dr. André Fenton at New York University (NYU) runs a lab in which he (along with other researchers at NYU) aims to “[investigate] the role of the hippocampus in controlling how we choose relevant information to process” by “studying the interaction of memories and neural activity in signaling information from multiple spatial frames.” In a landmark experiment with Dr. Todd Sacktor, Dr. Fenton identified “protein kinase M zeta (PKMzeta) as a key molecular component of long term memory.” When PKMzeta is selectively inhibited in specific brain areas, long-term memories are erased for “even a month after rats learn a place avoidance task.”
More specifically, when PKMzeta is inhibited, “place cells lose their spatial firing specificity.”
In short, then, rats that have been trained to avoid certain locations in a small chamber will no longer be able to (or remember to) avoid them because the rats’ place cells fail to properly communicate location-based information within their brains.
To these rats, tasks that were once practically inherent and familiar are now impaired and brand-new.
While this research has yet to be applied in humans, the wide-ranging implications of being able to essentially reset memory warrants ethical consideration. Let’s imagine that “one day we can create a drug that's really focused-- that can take out specific kinds of memories.” In what situations could we use this drug clinically? Who would be permitted to use it? What kinds of regulations would need to be in place? And, most importantly, what does it mean to allow human beings to selectively “delete” certain memories over others?
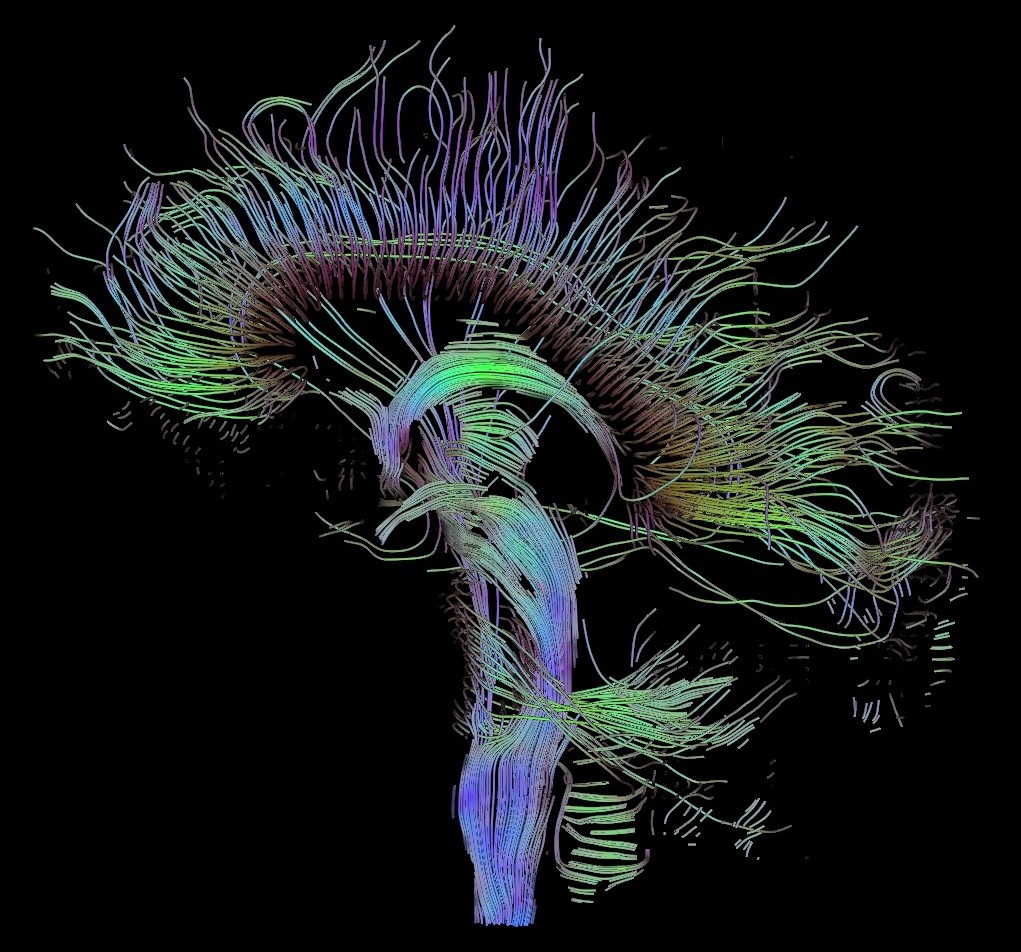
 |
| A tractographic reconstruction of some of the many neural connections in the human brain. (Image courtesy of Wikipedia.) |
About 150 years after Julius Aranzi gave a name to the hippocampus, Scottish philosopher David Hume published his novel A Treatise of Human Nature. In this book, Hume famously argued a then-radical idea of human nature and identity: “that the ‘self,’ as we conceive of it, is not a single spiritual or psychological entity, like a ‘soul,’ but rather a collection of discrete sensations and impressions — a bundle.” Linked together, these “bundles” create a distinctive and unique “self” that separates us human beings from one another. The key to Hume’s argument is the identity of these linkages between bundles.
We call them memories.
In this view, memories, then, are at the center of what makes us distinctive and different individuals. They are what distinguish me from you, what constitute the core of our identities, and what separate the past from the present and the present from the future. As one philosopher said it, “life without memory is no life at all.” (This concept is why Alzheimer’s disease and other such progressive brain disorders are so widely feared in the modern world; by involuntarily tearing memories away, these diseases slowly strip individuals of their pasts and –many argue— of who they are.)
What, then, are the consequences to changing memories? If memories are what make us who we are, does removing or modifying or changing memories change who we are? If I can no longer recall the car accident that sent my mother into therapy for six years or the way I felt the day I was rejected from ten universities, am I still me? And, if I were still myself after these changes, how much would I have to modify my memory to alter who I am? A couple uncomfortable incidents? A dozen? All of them?
These questions have yet to be answered.
Still, “a lot of unpleasant, a lot of difficult memories,” bioethicist Art Caplan says, “form who we are. We learn. It becomes part of our character, our identity. Some might say the struggle against bad experiences is part of what makes us better people.” But, are there situations in which this hypothetical (although not purely hypothetical, as our discussion about place cells suggests) memory repression drug may prove useful?
 |
| "What if I told you that I could erase some of your memories? I'll just give you a pill, and poof, they're gone. Would you do it?" science web producer David Levin asks. (Image courtesy of Pixabay.) |
Many war veterans are plagued with nightmares and emotional trauma, often becoming prisoners to a disease we now call PTSD (post-traumatic stress disorder). Patients of this mental condition could benefit from having the option to break down memories that are the source of their disorders. This same logic could be extended to scores of torment and torture individuals. Targets of violent personal assaults. Victims of childhood trauma. Rape survivors.
In these circumstances, memory medication could offer individuals the promise of returning a great deal of his/her functioning prior to the traumatic incident. Rather than change who the person currently is, clinical applications to memory medication could restore who the person originally was.
But where do we draw the line? How do we determine if a memory is bad enough to warrant modification? And who determines if a memory warrants modification at all? Doctors? Patients? Law makers?
While advances in place cells and PKMzeta research are both far from allowing us the ability to selectively modify memory, these ethical considerations are relevant to any serious discussion regarding the future of the hippocampus as we know it.
Perhaps one day, the answers to these questions will help us tackle the biggest questions of all: can the sea monster-shaped structure in our brains someday shield us from the monsters of the real world?
Do we want it to?
References
Barry, Jeremy M., et al. "Inhibition of protein kinase M? disrupts the stable spatial discharge of hippocampal place cells in a familiar environment." Journal of Neuroscience 32.40 (2012): 13753-13762.
Baylis, Françoise. "'I am who I am': On the perceived threats to personal identity from deep brain stimulation." Neuroethics 6.3 (2013): 513-526.
Bir, Shyamal C., et al. "Julius Caesar Arantius (Giulio Cesare Aranzi, 1530–1589) and the hippocampus of the human brain: history behind the discovery." Journal of neurosurgery 122.4 (2015): 971-975.
Carey, Benedict. "Brain Researchers Open Door to Editing Memory." The New York Times. The New York Times, 05 Apr. 2009. Web. 08 Apr. 2017.
Gentile, Sal. “If we erase our memories, do we erase ourselves?” PBS, Public Broadcasting Service, 24 Nov. 2010. Web. 12 Apr 2017.
Hume, David. A treatise of human nature. Courier Corporation, 2003.
Levin, David. "Ethics of Erasing Memory." PBS. Public Broadcasting Service, 13 Jan. 2011. Web. 11 Apr. 2017.
Nadel, Lynn, and Morris Moscovitch. "Memory consolidation, retrograde amnesia and the hippocampal complex." Current opinion in neurobiology 7.2 (1997): 217-227.
Pastalkova, Eva, et al. "Storage of spatial information by the maintenance mechanism of LTP." science 313.5790 (2006): 1141-1144.
West, Mark J., et al. "Differences in the pattern of hippocampal neuronal loss in normal ageing and Alzheimer's disease." The Lancet 344.8925 (1994): 769-772.
Zimmer, Carl. "Memory researchers, rebuffed by science, came roaring back." STAT. STAT, 23 June 2016. Web. 09 Apr. 2017.
Want to cite this post?
Ramesh, Sunidhi. (2017). The [Sea] Monster Inside Me. The Neuroethics Blog. Retrieved on , from http://www.theneuroethicsblog.com/2017/04/the-sea-monster-inside-me.html

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}